


U.S. Department of
Health and Human
Sevices
National Institutesof Health
National Heart, Lung,and Blood Institute
Late GadoliniumEnhancement:Image Acquisition
Peter Kellman
Disclosures
I have no financial relationships to disclose.
- and -
I will discuss the following off label use in my presentation:
Use of contrast agent for late enhancement imaging
Peter Kellman, Ph.D., NHLBI/NIH
Late Enhancement Principle
Late Enhancement Principle
time
Normal Myocardium
Infarcted Myocardium
Ischemic but
Viable Myocardium
First-Pass
DelayedEnhancement
Gadolinium
contrast
injection
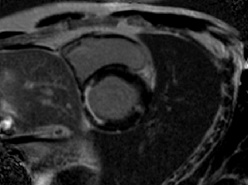
Late Gd Enhancement in Myocardial Infarction
Late Gd Enhancement in Myocardial Infarction
Acute MI
ruptured cell membrane
Chronic MI
collagen matrix
Normal
intact cell membrane
Mahrholdt H, et al. European Heart Journal. 2002; 23, 602–619.
Kim RJ, et al. Circulation. 1999;100:1992-2002.
Arheden H, Radiology. 1999 Jun;211(3):698-708.
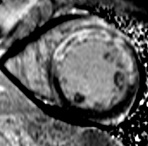
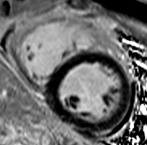
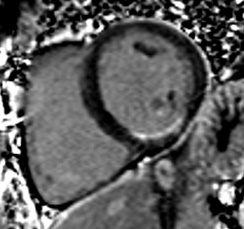
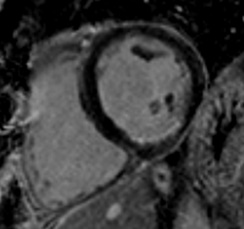
myocarditis with
mid-wall LGE
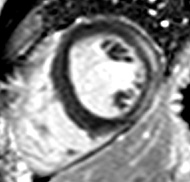
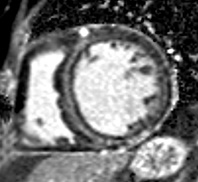
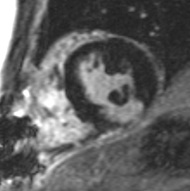
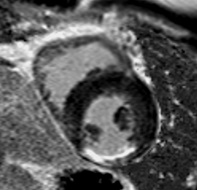
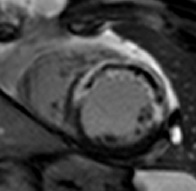
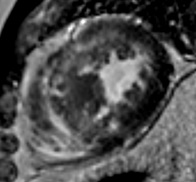
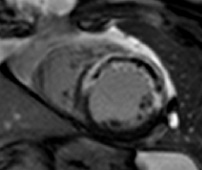
sub-endocardial
chronic MI
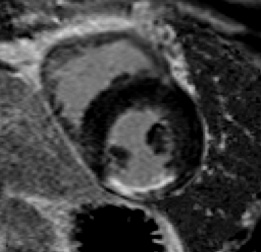
transmural
chronic MI
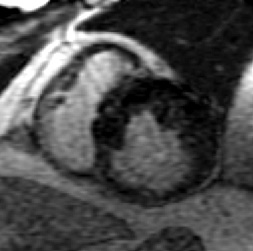
acute MI
with dark core
HCM with patchy LGE
myocarditis with
epicardial LGE
T1-weighting imaging sequences
Inversion recoveryInversion recovery
Saturation recovery
Steady state spoiled-GRE
Simonetti OP, et al., Radiology. 2001; 218:215-23.
•Extracellular agent which shortens T1
•Shorter T1 becomes bright on T1-weighted image
inversion recovery
time
signal
intensity
long T1
short T1
+
0
_
![ProtonBlurr1[1]](data/images/img15.gif)
![ProtonBlurr2[1]](data/images/img16.gif)
inversion recovery imaging
MI
Blood
normal
0
100
200
300
400
500
600
-1
-0.5
0
0.5
1
TI (ms)
null normal myocardium
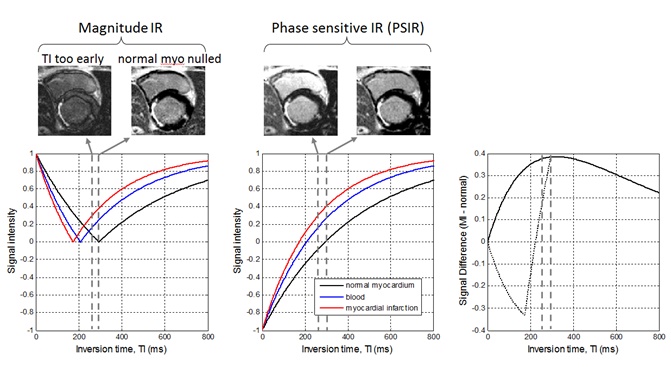
Inversion time insensitivity
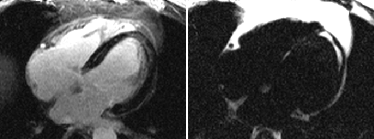
Magnitude images
Huber A, et al., Radiology. 2005 Dec;237(3):854-60.
Setser RM, et al., JMRI. 2005 May;21(5):650-5.
















Phase Sensitive images
inversion time
set early
inversion time
set late
normal
myocardium
nulled
inversion time
Kellman P, et al, Magn Reson Med. 2002 Feb; 47(2):372-83.
Typical Protocol (1.5T)
Gadolinium dose:0.1-0.2 mmol/kg
time from dose:10-20 minutes
pulse sequence:ECG gated (diastolic), segmented, turbo-FLASH
k-space acquisition: linear interleaved order
spatial resolution (typical):1.4 x 2 x 6 mm3 (256 x 135 matrix)
TE/TR/TI: 3.9/8.5/250-300 ms (adjusted to approx null normal myo)
bandwidth:140 Hz/pixel
imaging window:145-200 ms (17-23 views per segment)
IR preparation (non-selective):2 R-R
breath-hold duration:14-18 heart beats/slice (including 2 HB discarded acq)
(8-10 heart beats using 2x accelerated parallel imaging)
RF flip angle:25° IR image (PSIR PD image uses 5° reference)
Kim RJ, et al., JCMR. 2003;5(3):505-514.
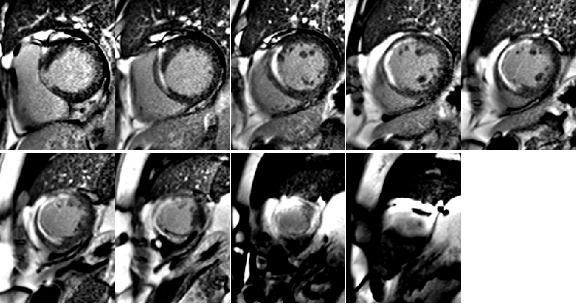
Setting Optimum Inversion TimeTI Scout Approach (SSFP IR cine)

95
200
305
408
120
225
330
435
148
253
355
460
173
278
383
488
Gupta A, Lee VS, Chung YC, Babb JS, Simonetti OP. Myocardial infarction: optimization ofinversion times at delayed contrast enhanced MR imaging. Radiology 2004;233:921–926.
2 R-R versus 1 R-R triggering
2 R-R inversions
1 R-R inversions
Using inversions every RR leads to incomplete magnetization recoveryand, therefore
•loss of SNR
•sensitivity to R-R variations -> artifacts
Single heartbeat late enhancement
•Rapid, multi-slice acquisition
•Arrhythmia insensitive
•Free-breathing acquisition
Huber A, et al., Investigative Radiology. 2006 Feb;41(2):148-53.
Huber A, et al., AJR. 2006 Mar;186(3):627-33.
Sievers B, et al., Circulation. 2007 Jan 16;115(2):236-44.
inversion
imagereadout
Kellman P, et al., MRM. 2004 Feb;51(2):408-12.

conventional
segmented with
poor breath-hold
single-shot
free breathing
Single Shot Pulse Sequence
EKG
R-wave trigger
180° inversion pulses
(delayed)
magnetization
single shot acquisition
(during mid-diastole)
1 2 3 4 N
1 2 3 4 N
IR data
(50° flip angle)
reference data
(8° flip angle)
pulse sequence:SSFP
k-space acq: ECG gated, single-shot
resolution:256 x 128
TE/TR: 1.2/2.7 ms
bandwidth:977 Hz/pixel
imaging window:172 ms
64 views using R=2
parallel imaging
RF flip angle:50° IR image (8° reference)
imaging duration:2 heart beats/slice
Motion corrected averagingfree-breathing late enhancement
accelerated
single shotacquisition
respiratorymotioncorrection
averaging
raw
motion corrected
Full FOV
zoom
parallel imaging
rate 2
Kellman P, et al., MRM. 2004 Feb;51(2):408-12.
Ledesma-Carbayo MJ, et al., JMRI. 2007. Jul; 26(1):184-190


Conventionl
IR-turboFLASH
breath-held
accelerated single-shot
IR-SSFP
free-breathing
single frame
16 HB
single frame
2 HB
8 averages
16 HB
motion
corrected
same acquisition time
Respiratory Motion Corrected Averaging:
Selective averaging ~ 50% of “best” frameseffectively mitigates thru plane motion
Rate 3 with 256x144 matrix
motion corrected
average
single heart beat
images
motion corrected
Free-breathing PSIR LGE
9-slice, 4 repetition MOCO average
72 s for SAX stack
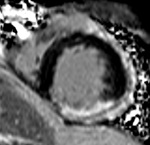
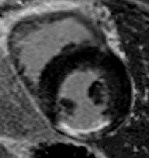
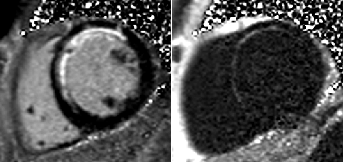
MI-to-blood pool contrast
good contrast MI-to-blood
poor contrast MI-to-blood
10 min
20 min
time from Gd administration
Intramyocardial Fat:may lead to false late enhancement
WATER
FAT
conventional PSIR
late enhancement
multi-echo PSIR
fat/water separated
late enhancement

apparent lateenhancement
inversion time(TI)
magnetization
normal
MI
fat
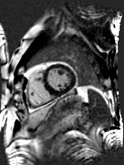
Chronic MI Patient:Fibro-fatty infiltration
Fatty
infiltration
MI
WATER
FAT
1 2 3 M
N-echoes per PE line
IR data
(25° flip angle)
reference data
(5° flip angle)
multi-echo PSIR GRE sequence
Review
Review
•Gd-DTPA extra-cellular contrast agent
• normal and fibrotic tissue have different kinetics
•T1-weighted imaging
• inversion recovery (IR)
• segmented FLASH or single-shot SSFP
• TI scout or phase sensitive IR (PSIR)
•Single Shot, Respiratory Motion Corrected Averaging
•Fat-water separated late enhancement
time

DelayedEnhancement
Gadolinium
contrast
injection

Gd washout